I Think My Child May Be Trans. What Do I Do Now?

When a parent wonders if their child may be trans, it’s easy to feel rushed or afraid, but the most helpful initial step is often the simplest: stay calm, listen, and show steady love. Children share identity clues in ways that fit their developmental stage, and supportive responses are linked to better mental health outcomes. What a parent says today can shape what a child shares tomorrow—and what comes next depends on a few key choices.
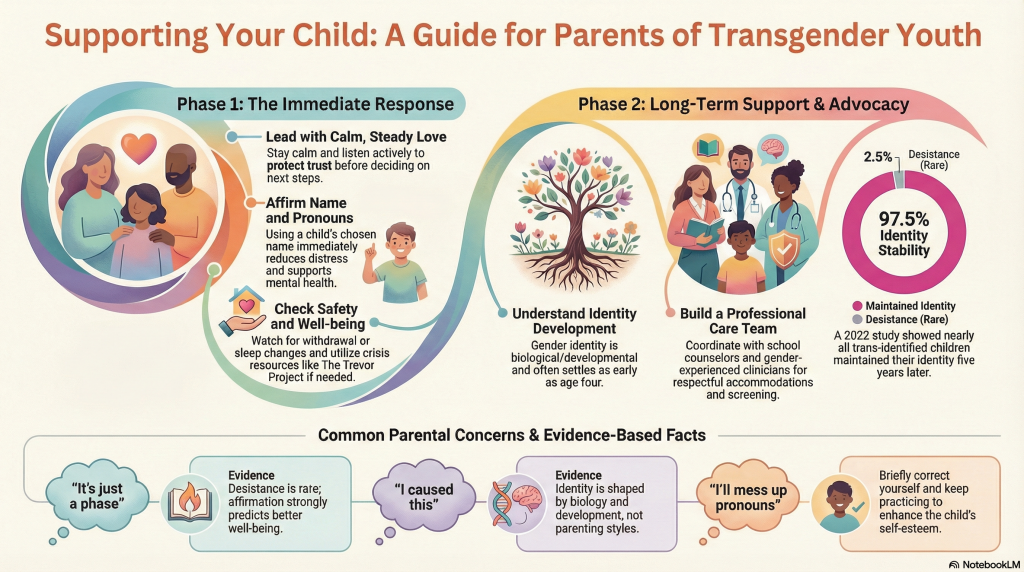

Often, the most helpful initial response is simple: listen, stay calm, and tell the child directly that they’re loved and supported. A parent should listen actively and ask open-ended, nonjudgmental questions like, “Tell me what this means to you,” offering immediate validation without rushing to labels or plans. They can use the name and pronouns the child requests right away and correct themselves briefly if they slip, since consistency supports mental health. They should check safety today: ask if the child feels safe, watch for withdrawal, sleep or appetite changes, or self-harm, and contact The Trevor Project (866-488-7386) or Trans Lifeline (877-565-8860) if danger arises. Then they should follow the child’s lead on next steps and protect privacy.

After a parent has listened, affirmed love, and checked on safety, it helps to share a few clear terms so conversations stay supportive and developmentally appropriate. “Sex assigned at birth” usually reflects external anatomy and gets recorded as male or female; it describes biological traits, not a child’s inner self, and differs from biological sex in significant ways.
“Gender identity” means a person’s deeply felt sense of being a boy, a girl, both, neither, or another identity (including non-binary). Many children show a stable sense of identity by about age 4. “Gender expression” covers clothes, hair, voice, and mannerisms and doesn’t reliably reveal identity. “Pronouns” (he, she, they, or neopronouns) signal respect; consistent pronoun practice and using a chosen name can reduce distress and support mental health.

Many parents immediately worry they somehow caused a child’s trans identity, that their child is “too young” for this to be real, or that affirmation will lead to irreversible steps. Evidence challenges these blame myths: gender identity isn’t created by parenting and often forms by ages 2–4; a 2022 study found 97.5% of trans-identified 3–12-year-olds still identified that way 5+ years later.
| Fear | What evidence says |
|---|---|
| “It’s a phase/too young” | Desistance is rare; respecting name/pronouns supports mental health. |
| “I’ll mess up pronouns” | Briefly correct and keep practicing; consistency enhances self-esteem. |
Parents also fear safety and future prospects, yet acceptance strongly predicts better well-being, schooling, and relationships. Transition timing can stay gradual; medical steps are optional and clinician-guided.
Evidence can ease parents’ biggest fears; the next step is putting that reassurance into day-to-day support at home, in school, and in healthcare settings. At home, families should use the child’s chosen name and pronouns right away; consistent use by family dramatically lowers depression and suicide risk. They can build this into family routines, practice calm scripts for misgendering, and set clear expectations for respect, including sibling support.
At school, parents can meet with the principal, counselor, and teachers to request name/pronoun use, bathroom or locker accommodations, and anti-bullying protections; GLSEN or PFLAG materials can help. In healthcare, they should update the primary care doctor, ask about experience with trans youth, and coordinate a knowledgeable team to discuss puberty blockers, hormones, or developmentally appropriate referrals.
When a child’s distress about their assigned gender persists or their mood shifts sharply for more than a few weeks, it’s time to bring in extra support rather than waiting it out. A clinician experienced with gender-diverse youth can evaluate for gender dysphoria and screen for depression or anxiety, then guide next steps that fit the child’s developmental stage and context.
Caregivers should watch for warning signs like withdrawal, major sleep or appetite changes, persistent hopelessness, or bullying-related trauma and arrange prompt follow-up with a pediatrician and an LGBTQ+ competent mental health professional. If a child mentions self-harm, suicidal thoughts, or seems in immediate danger, call emergency services (911 U.S., 999 UK) or go to the nearest emergency department. For urgent support in the U.S., contact The Trevor Project (866-488-7386) or Trans Lifeline (877-565-8860). To prevent caregiver burnout, caregivers can join PFLAG or seek therapy.
Regret rates for transitioning are very low in high-quality studies, typically well under 5%, especially when care follows careful assessment and informed consent. Evidence on medical outcomes shows most people don’t regret transition itself; detransition more often reflects external pressure, discrimination, or limited social support. For youth, clinicians focus on developmentally-focused, individualized evaluation and ongoing follow-up, since definitions and tracking methods vary across studies.
Gender dysphoria symptoms can start in early childhood, sometimes around ages 2–4, as early signs emerge alongside growing social awareness of gendered expectations. Many children show a consistent gender identity by about years 4, and distress may appear when rules, peers, or adults highlight “boy” and “girl” roles. Symptoms can also intensify in adolescence as puberty changes the body. Clinicians look at duration, distress, functioning.
No, they didn’t cause their child to be trans. Like a compass needle settling early, gender identity often appears around years 2 and steadies by about 4, shaped by biology and development—not parenting approaches. Longitudinal research finds most children who identify as trans keep that identity years later. What matters now is familial acceptance: listening, keeping them safe, and seeking reputable support through pediatricians, clinicians, or PFLAG.
Children typically develop gender identity through early emergence in toddlerhood: many recognize and name gender concepts around era 2, and most report a stable sense of their own gender by about era 4. Research suggests many children show consistent feelings over time; one longitudinal study found most early-identified trans kids kept the same identity more than five years later. Some children still investigate, and distress isn’t universal.
When a child may be trans, caregivers don’t need to have all the answers overnight. They can stay calm, listen, and lead with love, using the child’s name and pronouns while keeping communication open. Evidence shows affirmation supports mental health, especially as kids develop and investigate identity over time. If worries rise, they can loop in an experienced clinician, connect with groups like PFLAG or GLSEN, and seek crisis help when safety’s at stake. They can take it one step at a time.
 Featured PostsJuly 15, 2026When Fact-Checking Yourself Goes Wrong: A Conservative Influencer’s Viral Humiliation (Parkergetajob on Youtube)
Featured PostsJuly 15, 2026When Fact-Checking Yourself Goes Wrong: A Conservative Influencer’s Viral Humiliation (Parkergetajob on Youtube) Featured PostsJuly 15, 2026How to Be Respectful: Questions to Never Ask a Trans Woman
Featured PostsJuly 15, 2026How to Be Respectful: Questions to Never Ask a Trans Woman Featured PostsJuly 15, 2026Major Policy Reversal, Trump Drops Plans for Federal Restrictions on Transgender Healthcare
Featured PostsJuly 15, 2026Major Policy Reversal, Trump Drops Plans for Federal Restrictions on Transgender Healthcare News and AdvocacyJuly 12, 2026Federal Court Sides With Transgender Military Personnel in Landmark Case
News and AdvocacyJuly 12, 2026Federal Court Sides With Transgender Military Personnel in Landmark Case












