Why Are Hospitals Still Asking This? The Legacy Inquiry Driving Medical Disparities
You fill out the form, you cross out the label, you explain your family again. In many hospitals, “Mother” and “Father” fields still treat one family structure as the default. You observe how that choice burdens LGBTQ parents, stepparents, adoptive parents, and guardians with extra proof at moments when care should come first. Evidence shows intake design shapes access, delays, and trust—and one simple wording change can expose a much larger problem.
When a hospital intake form asks for “Mother” and “Father,” it does more than collect information: it tells families which relationships the institution expects to see. You can see assumed kinship built into the boxes: one woman, one man, usually biological, usually married. That template doesn’t match many LGBTQ families, including lesbian couples, gay dads, nonbinary parents, single parents, and blended households. When your family doesn’t fit, the form turns ordinary intake into language erasure. It makes one parent legible and pushes another to the margin, sometimes literally. Evidence from hospitals and public systems shows these labels persist because institutions inherited a postwar nuclear-family period. You’re not facing a neutral form; you’re facing design that quietly ranks families by proximity to an outdated norm.
Although a form may look routine, it can force LGBTQ and nonbiological parents to defend a relationship other families get to simply state. When one encounters only “mother” and “father,” one must decide whether to cross out labels, squeeze your name into a margin, or explain your family to staff who may still question you. That isn’t a harmless clerical step; it’s an administrative burden that turns care into a test of legitimacy.
In hospitals, that burden carries practical stakes. If intake systems don’t recognize you as a parent or guardian, you may face delays, repeated questions, or confusion during handoffs. Those moments matter, especially when a child needs emergency access and you’re trying to focus on care, not proving that you belong there.

That pressure to prove parenthood doesn’t end once staff accept your explanation. If you’re a nonbiological parent, love and daily caregiving may not carry legal weight. In urgent care, staff may need custody documentation before they let you authorize treatment, access records, or provide emergency consent.
| Situation | What you may need | Equity impact |
|---|---|---|
| ER visit | Court order | Delays care |
| School call | Adoption decree | Questions authority |
| Insurance issue | Birth certificate | Blocks access |
| Travel emergency | Guardianship papers | Raises scrutiny |
You shouldn’t have to keep a legal file beside the diaper bag. Yet many families do, because systems often treat biology as proof and caregiving as insufficient. That standard burdens LGBTQ parents, stepparents, and kin caregivers disproportionately.
Because family law and health administration differ across the U.S., inclusive forms often depend on where you live and which institution you enter. You can see policy variation in how states interpret parentage, birth certificates, and hospital compliance after marriage-equality rulings. States such as California, New York, Vermont, and Colorado have clearer protections, while others leave more discretion to local systems. That discretion matters. A well-funded urban hospital may update electronic records, train staff, and audit intake language. An under-resourced rural clinic may rely on old templates for years. These funding disparities turn paperwork into another access gap. You shouldn’t need the “right” ZIP code to have your family recognized, but uneven law, technology budgets, and leadership priorities make recognition inconsistent across care settings.
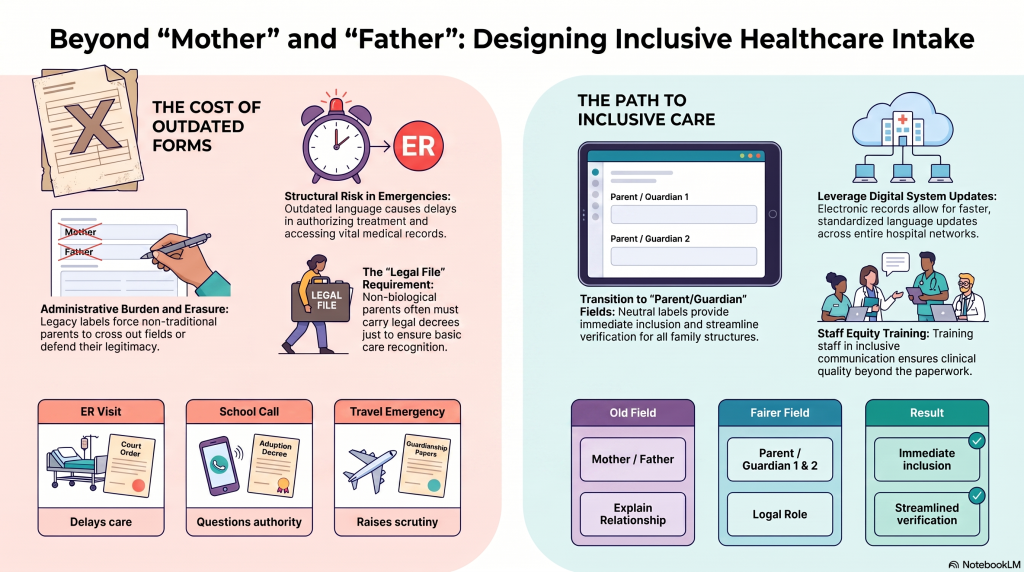
At the point of intake, replacing “Mother” and “Father” with “Parent/Guardian” or “Legal guardian 1” and “Legal guardian 2” makes recognition automatic rather than conditional. You don’t force a lesbian mom, single dad, grandparent, or nonbinary parent to explain themselves before care begins.
| Old field | Fairer field | Result |
|---|---|---|
| Mother | Parent/Guardian 1 | Immediate inclusion |
| Father | Parent/Guardian 2 | Fewer corrections |
| “Explain relationship” | Legal role | streamlined verification |
These gender neutral labels align paperwork with law, caregiving reality, and patient safety. You give staff clear authority signals, reduce repeated questioning, and limit emotional labor for families already under stress. Evidence-based equity starts here: design forms for the families who actually arrive, not the template institutions inherited.
Yes, you can request form corrections before appointments. Ask the clinic portal team, registration desk, or patient relations for correction requests and preappointment edits to names, guardians, pronouns, emergency contacts, and relationship labels. You shouldn’t have to explain your family repeatedly. Evidence shows outdated fields create administrative burden and exclusion, especially for LGBTQ and nonbiological parents. If staff refuse, ask for a supervisor and document the request in writing.
Hospital administrators usually decide intake form wording, but they rely on compliance teams, electronic health record vendors, clinicians, policy makers, and sometimes patient advocates. You should ask who owns registration forms, because decisions often sit with operations or legal departments. Evidence shows wording shapes access and dignity, so equity-focused review matters. You can push for Parent/Guardian language, request correction pathways, and urge hospitals to involve affected families before forms go live.
Yes—digital forms are usually easier to update than paper forms because you can push digital updates across systems, track version control, and standardize inclusive language quickly. But ease depends on funding, vendor limits, staff training, and leadership. You still need equity-focused review to replace “Mother/Father” with “Parent/Guardian” fields. Paper forms require reprinting; digital forms require governance, testing, and accountability so changes actually reach every patient.
You train staff like lives depend on every word. Start with Pronoun training, scripted intake practice, and Bias workshops tied to real patient scenarios. You audit interactions, not just forms, because evidence shows exclusion persists when staff address only biological parents. You teach “parent,” “guardian,” and “caregiver” as defaults, then coach corrections without defensiveness. You measure complaints, update EHR prompts, and reward inclusive communication as core clinical quality.
Ask staff to pause care decisions and escalate immediately. You should calmly present legal documents again, request advocacy from a patient advocate, charge nurse, or social worker, and ask them to document the refusal. If resistance continues, seek ombudsman support, hospital legal/risk management, or an administrator. You’re protecting your youngster’s access to care and challenging inequitable assumptions. Afterward, file a written complaint and share copies with relevant agencies.
When you see “Mother” and “Father” on a hospital form, you’re seeing a locked door where care should have a welcome mat. One two-dad family may spend critical minutes proving who can consent while a child waits. That delay isn’t sentimental; it’s structural risk. If you replace those fields with “Parent/Guardian 1” and “Parent/Guardian 2,” you don’t erase anyone. You make verification clearer, emergencies safer, and care more equitable for every family.
 Featured PostsJuly 31, 2026A Guide to Bilateral Orchiectomy as Gender-Affirming Care
Featured PostsJuly 31, 2026A Guide to Bilateral Orchiectomy as Gender-Affirming Care News and AdvocacyJuly 30, 2026Artificial Outrage: When Conservatives Use AI to Invent the Trans Threat They Can’t Find
News and AdvocacyJuly 30, 2026Artificial Outrage: When Conservatives Use AI to Invent the Trans Threat They Can’t Find Featured PostsJuly 26, 2026Your Journey from Female to Male: An Introductory Guide to Phalloplasty
Featured PostsJuly 26, 2026Your Journey from Female to Male: An Introductory Guide to Phalloplasty Featured PostsJuly 26, 2026When a Child Says They’re Trans: a Deep Dive Into Pediatric Care and Family Decisions
Featured PostsJuly 26, 2026When a Child Says They’re Trans: a Deep Dive Into Pediatric Care and Family Decisions