Transgender Women Exhibit Brain Sex Profiles Shifted Toward Their Gender Identity

If you treat “brain sex” as a multivariate MRI pattern rather than a binary label, you get a more precise question: where do transgender women fall before hormone therapy? In this study, they didn’t align fully with cisgender men or cisgender women. Their scores shifted toward the female-typical range on a continuous index trained from population data. That result is suggestive, not decisive, and its limits matter as much as its implications.
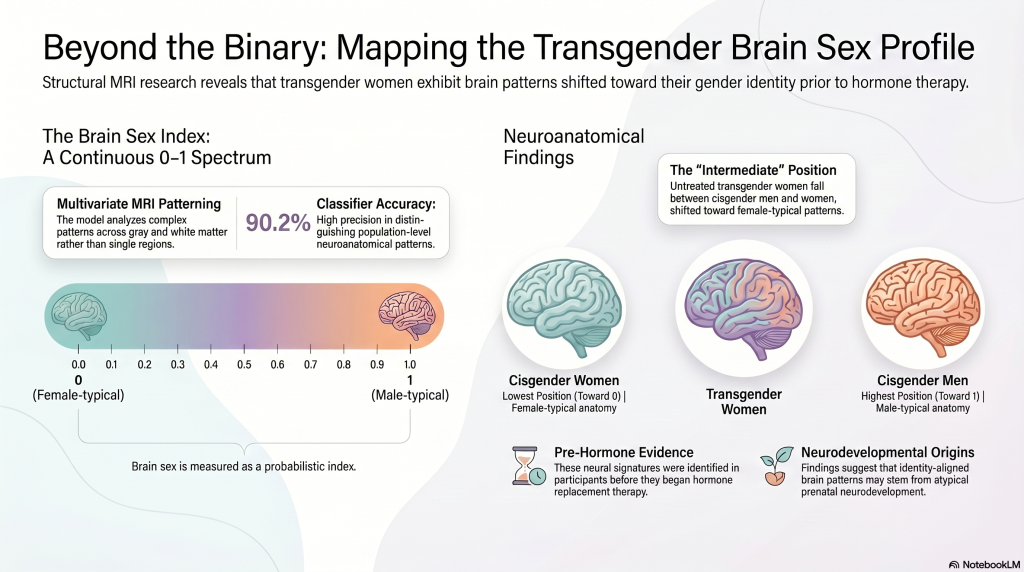
Here, “brain sex” doesn’t mean a single male-or-female brain feature; it means a probabilistic MRI-based index that estimates where an individual’s whole-brain anatomy falls on a continuum from 0 (average female) to 1 (average male).
You should read it as a multivariate summary, not a biological essence. The researchers trained Relevance Vector Regression on 547 independent MRI scans, using PCA-reduced patterns of gray and white matter after smoothing, normalization, and resampling to 4 mm voxels. Validation metrics were strong, so the score estimates how closely a person’s anatomy resembles population-average male versus female patterns. Because it’s continuous, distributed, and population-referenced, it avoids simplistic binary labeling. That framing matters for neuroethical implications and public misinterpretation: you can’t infer identity, destiny, or any single-region “male brain” claim from this metric alone.

Using the MRI-based Brain Sex index, the researchers found that transgender women, scanned before hormone therapy, occupied an intermediate position between cisgender men and cisgender women. You can read this as a measurable shift toward female-typical neuroanatomical patterning, though not a complete overlap with cisgender women. Overall group differences were robust (F(2,69)=40.07), and transgender women differed markedly from cisgender men (p=0.016) and cisgender women.
| Group | Finding |
|---|---|
| Transgender women | Intermediate, shifted femaleward |
| Cisgender controls | Clear male-female separation |
Because classifier accuracy stayed high, the pattern likely reflects subtle multivariate anatomy, not model failure. Analytically, this supports altered neurodevelopmental trajectories and possible prenatal hormonal influences, while still showing closer proximity to cisgender men. You should treat the result as suggestive, not definitive, pending larger independent replication studies.

To understand why transgender women fell between cisgender male and female groups, you need to look at how the study quantified “brain sex.” The researchers trained a relevance vector regression (RVR) model on PCA-reduced structural MRI data from an independent IXI dataset of 547 adults, with sex coded on a continuous scale from 0 for female to 1 for male.
You can think of this MRI classifier as learning multivariate patterns across gray and white matter. T1-weighted MPRAGE scans underwent normalization, tissue segmentation, smoothing, and resampling to 4 mm voxels before extraction of PCA features. Researchers then applied the same PCA transformation to 24 cis men, 24 cis women, and 24 transgender women. The trained model generated each person’s Brain Sex index. Validation showed 90.2% cross-validated accuracy and 88.3% control-sample accuracy, with AUC 0.97.
Rather than forcing every scan into a male-or-female box, the researchers treated brain sex as a continuous trait because neuroanatomy shows substantial overlap, individual variation, and mixed sex-typical patterns across regions. You can see that choice in their multivariate relevance vector regression model, trained on an independent IXI sample, which generated a Brain Sex index from 0 to 1 instead of a hard label.
That design preserves statistical nuance. A binary classifier would collapse intermediate anatomies and hide partial shifts that transgender studies often report across different structures. By using a continuum, you can quantify mixed patterns and test whether values fall between cisgender male and female distributions. The resulting framework also fits multifactorial biology—genes, prenatal hormones, and development don’t produce perfectly discrete categories—and it carries ethical implications, too, for interpretation.
That continuous Brain Sex index sharpens the study’s main claim, but it also sets clear limits on what the data can support. You can say the MRI classifier, trained on 547 independent adults, detected a statistically reliable intermediate pattern in untreated transgender women: their Brain Sex scores fell between cisgender men and cisgender women, with significant group differences overall and versus cisgender men.
You can also infer that this probabilistic shift appears independent of adult cross-sex hormones, because participants were scanned before therapy and were SRY-positive. But you can’t claim causation. The cross-sectional design and small transgender sample can’t identify developmental origins, mechanisms, or timing. You also can’t generalize broadly beyond pre-hormone transgender women. Clinical implications remain tentative until larger, more diverse replication studies establish reproducibility and effect stability.
Yes, hormone therapy can change these brain patterns over time, though effects vary by region, duration, life stage, and baseline biology. You’d expect hormone influence on cortical thickness, white matter microstructure, connectivity, and functional responses, based on neuroplastic mechanisms. Evidence suggests longitudinal changes emerge across months to years, but causality remains complex because studies differ in design, sample size, imaging methods, and confounding factors. Stronger longitudinal data are still needed.
No, you don’t perceive transgender men included here; you observe transgender women analyzed, cisgender controls compared, and neural patterns interpreted. That matters for transgender inclusion because the sample limits what you can generalize across trans populations. From an evidence-based, analytical view, study limitations are clear: the design can characterize findings in transgender women, but it can’t test whether transgender men show similar, distinct, or hormone-responsive brain patterns over time.
You’d describe the sample size as modest and the demographic diversity as limited. The study included 24 transgender women and 24 cisgender men, giving you 48 participants total. That supports controlled group comparisons, but it restricts statistical power and generalizability. You also don’t see broad demographic diversity reported, such as varied ethnic, socioeconomic, or geographic backgrounds. So, you should treat the findings as preliminary rather than broadly representative across populations studied.
Could you identify gender identity from a scan alone? No, you can’t. Brain imaging may reveal population-level neural markers associated with gender identity, but it doesn’t provide a definitive individual diagnosis. You’d face major limits from overlap across groups, small effects, and methodological variability. You’d also need to weigh serious legal implications, because misclassification could affect privacy, discrimination, and autonomy. Evidence supports patterns, not deterministic identification for individuals.
You face several ethical concerns in brain sex research involving transgender communities: Informed consent, Privacy risks, stigmatization, and misuse of findings. Researchers must explain limits, uncertainties, and potential harms clearly, because scans can’t validate identity. You also risk data breaches, re-identification, and discriminatory interpretation by clinicians, employers, or policymakers. Ethical practice requires community involvement, transparent methods, careful communication, and safeguards that prevent pathologizing transgender people or undermining autonomy.
You should read this study as a calibrated signal, not a verdict. The MRI-derived brain-sex index places transgender women, before hormones, between cisgender male and female reference patterns, shifted toward their gender identity. That result supports a distributed, nonbinary model of brain sexual differentiation rather than a simple either-or map. But, like Plato’s shadows, it reflects correlation, not essence: population-trained prediction can suggest altered neurodevelopmental trajectories, yet it can’t establish cause, mechanism, or individual certainty.
 News and AdvocacyJuly 6, 2026Federal Judge Shuts Down Trump Administration’s Push for Trans Kids’ Medical Files
News and AdvocacyJuly 6, 2026Federal Judge Shuts Down Trump Administration’s Push for Trans Kids’ Medical Files Featured PostsJuly 3, 2026Solitude, Not Silence: My Foundations for Living Alone
Featured PostsJuly 3, 2026Solitude, Not Silence: My Foundations for Living Alone Featured PostsJuly 3, 2026What Is Gender Affirming Care?
Featured PostsJuly 3, 2026What Is Gender Affirming Care? Featured PostsJuly 3, 2026Connecting the Dots: Often-Overlooked Signs of Being a Trans Woman
Featured PostsJuly 3, 2026Connecting the Dots: Often-Overlooked Signs of Being a Trans Woman