MTF Bottom Surgery: My SRS/GCS Journey, Care Tips, and Life After Healing

At 3 a.m. on your second dilation, the process can feel less like a finish line and more like calibrating a finely tuned instrument. If you’re considering MTF bottom surgery, you need more than hope; you need clear facts about dysphoria, preparation, pain control, wound care, sensation, and sex after healing. This account stays clinical and honest about what changes, what improves slowly, and what can still surprise you months later.
What tipped me toward MTF bottom surgery was the persistence of my dysphoria: it wasn’t occasional discomfort, but a near-daily sense that something was fundamentally wrong, especially during sex and in the guilt and shame that often followed orgasm.
You recognize that this is about gender identity and emotional alignment, not sexual augmentation. You weigh evidence carefully: JAMA Surgery reported 44% lower suicidal ideation and 42% less psychological distress after gender-affirming surgery, while reviews show reduced dysphoria and greater body satisfaction. You prioritize body consonance, ordinary ease, and less fear of being outed. You also keep expectations realistic: surgery can support self-acceptance, but it isn’t a cure-all. Practical choices matter too, yet your decision clarity comes from sustained distress, informed judgment, and adequate social support around you.

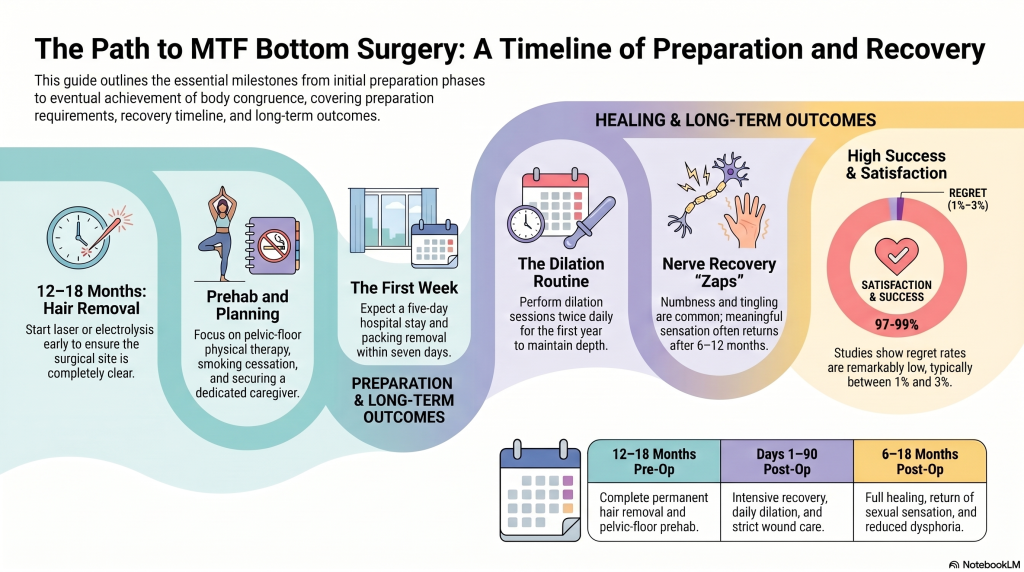
Once I felt confident that surgery matched my long-term needs, I shifted from deciding to preparing. You should start hair removal 12 to 18 months before surgery, using laser or electrolysis, and confirm your surgeon’s clearance standards so no hair remains inside the neovagina. Pre op counseling also helps you understand expectations, consent, and practical planning.
You’ll also strengthen recovery by treating preparation like prehab. Pelvic-floor physical therapy, better nutrition, and stopping smoking can support healing and lower complication risk. Follow your surgeon’s hormone instructions carefully, and disclose all substance use to anesthesia staff. Plan logistics early: a five-day hospital stay, nearby lodging, caregiver help, transportation, time off work, and wardrobe adjustments. Learn dilation and wound-care steps beforehand so the routine won’t feel unfamiliar after surgery later.

Although recovery unfolds in stages, the initial three months after MTF bottom surgery are usually the most demanding, with a hospital stay of about five or more days, packing removal around day five to seven, and dilation quickly becoming the center of your daily routine.
You may also notice hormone shifts, changing libido, pelvic-floor tension, and emotional adjustment needs during healing.
As healing becomes less all-consuming, many people start noticing how sex, arousal, and everyday sensation feel different after surgery. Early on, you may feel numbness, tingling, or brief “zaps” as nerve regrowth progresses. Sensation usually returns slowly, often over six to twelve months or longer, so changes can be uneven.
Orgasm can still happen because the neoclitoris retains sensitive nerve endings, though pleasure may feel different in intensity, location, or buildup. Your libido may also shift as hormones change and dysphoria eases. Because a penile-inversion neovagina doesn’t self-lubricate, you’ll usually need lubricant for dilation, toys, or sex. Penetration often requires patience, pelvic floor retraining, and consistent dilation. Most surgeons advise waiting about twelve weeks before internal exploration, and partner communication makes comfort, pacing, and consent much easier.
By the time full healing settles in—often somewhere between six and eighteen months or longer—you may feel a major shift in daily life: less gender dysphoria, more physical ease, and far less vigilance about being seen or outed. That often means reduced dysphoria, greater comfort, and real social freedom.
As full healing settles in, daily life often opens into less dysphoria, more ease, and greater social freedom.
You may also notice higher body confidence and less sexual shame. Still, adjustment isn’t linear; occasional doubt can persist during the initial post-op year for many patients.
After MTF bottom surgery, you’ll stay hospitalized about five days with packing, a stent, and a catheter initially. You’ll start diligent dilation, usually twice daily, plus saline or Betadine rinses, careful drying, and antibiotic powder. Use water-based lubricant because your neovagina won’t self-lubricate. You’ll need follow-up for depth, width, and complications, along with pelvic physiotherapy and scar management to support healing, function, and comfort over time.
You’ll find regret after MTF bottom surgery is low, typically about 1% to 3% in medium-term studies. Most patients report improved body satisfaction, and satisfaction metrics are generally high. When regret happens, it often relates to complications, limited support, unmet expectations, or identity changes. You can lower risk through thorough decision counseling, realistic preparation, strong mental-health support, and choosing an experienced surgical team.
You’ll usually see full healing around 12 months, though recovery unfolds in stages. Imagine this: the initial 90 days do most of the heavy lifting, with strict rest, dilation, and wound care shaping outcomes. You’ll leave the hospital in about 5–7 days, but sexual sensitivity often improves after 6 months and can keep changing for 18 months. Pelvic therapy can support comfort, function, and confidence during recovery.
If you’re considering MTF bottom surgery, you deserve clear expectations, skilled support, and patience with healing. Your recovery won’t be linear, but steady care—especially dilation, pelvic relaxation, and follow-up—can protect long-term function and comfort. One review found regret rates after gender-affirming surgery were under 1%, far lower than many other major procedures, which adds useful perspective but doesn’t replace personal readiness. When your decision is grounded, preparation and self-compassion can make life after healing feel deeply congruent.
 Featured PostsMay 5, 2026MTF Bottom Surgery: My SRS/GCS Journey, Care Tips, and Life After Healing
Featured PostsMay 5, 2026MTF Bottom Surgery: My SRS/GCS Journey, Care Tips, and Life After Healing Featured PostsMay 5, 2026Can Anyone Explain Gender Fluid Identity to Me?
Featured PostsMay 5, 2026Can Anyone Explain Gender Fluid Identity to Me? News and AdvocacyMay 1, 2026What’s Behind the Right’s Fixation on Trans People
News and AdvocacyMay 1, 2026What’s Behind the Right’s Fixation on Trans People Featured PostsMay 1, 2026Am I Non-Binary? Questions to Help You Discover Your Gender Identity
Featured PostsMay 1, 2026Am I Non-Binary? Questions to Help You Discover Your Gender Identity











