The Idol in the Mirror: How the Ego Obscures the Trans Self

Like Narcissus at the water’s edge, you can start confusing the reflection with the self. In a culture that rewards strong narratives and flawless “after” photos, it’s easy for your trans identity to shift from lived experience into something you must perform and defend. Over time, that performance can bury trauma, complicate dysphoria, and silence doubt—while still looking “empowered” from the outside. The real cost of that split often shows up later, in ways you don’t expect.
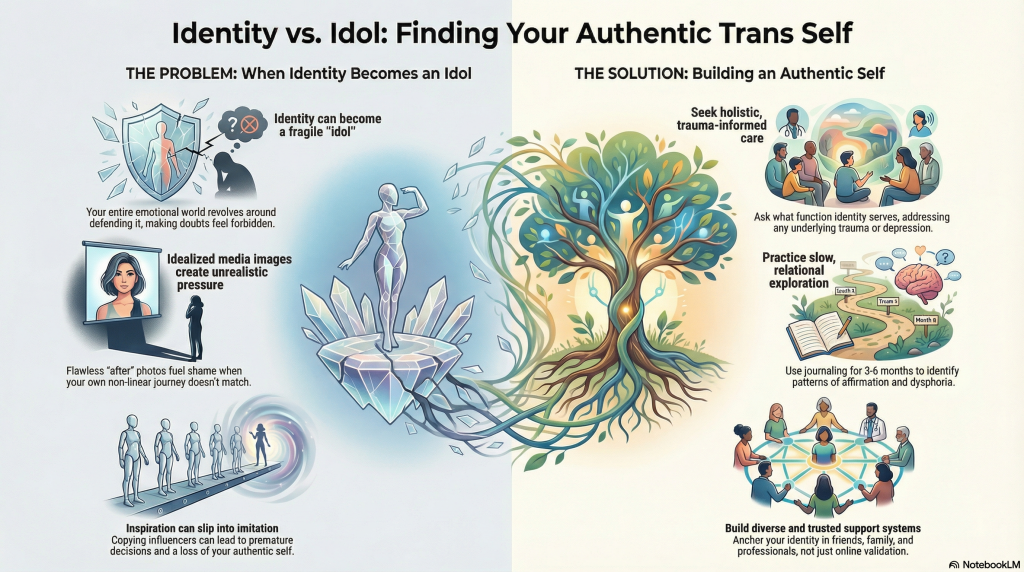

When a trans identity starts functioning like an idol, the core problem isn’t that someone names or honors their gender experience, but that they begin to organize their entire emotional world around protecting that identity at all costs. You may feel compelled to maintain a perfectly coherent narrative, even when your mood, body image, or sense of self shifts.
Under intense social reinforcement—likes, praise, community status—ordinary doubts can feel dangerous, so you double down. Identity fixation can then obscure trauma, depression, or neurodivergence that also need care. Clinicians describe cases where change becomes the only imagined solution, even when distress persists. A trauma‑informed, holistic approach invites you to ask what functions your identity serves and to anchor worth in more than one story about who you are.

Scrolling through streams of flawless before‑and‑after photos and celebrity transformations stories, you’re not just “seeing what’s possible”; you’re absorbing powerful templates for what a “real” or “successful” trans life is supposed to look like. Research on social comparison shows that these curated benchmarks can quietly raise the bar for your body, timeline, and “outcome,” often increasing dysphoria and shame when you don’t match them.
Those polished timelines aren’t just inspiration; they quietly rewrite what your transition is “supposed” to be
Clinically, hormone and surgical results vary widely, but feeds rarely show that nuance. Instead, you may start organizing your identity around an idealized persona, introjecting their aesthetics, goals, even language.

Even genuine admiration for another trans person can quietly slide into imitation that pulls you away from yourself. You may start with mirroring behaviors—copying a name, style, pronouns, or even medical choices—before you’ve traced your own history of dysphoria or investigated slower, reversible steps. Research with detransitioners shows that social pressure and identity exploration, not always stable trans identity, often drive premature decisions.
Clinically, this can become identity foreclosure: your ego latches onto a trans persona as a rescue from shame or isolation, cutting off other possibilities before you’ve fully evaluated them. Qualitative studies describe people abandoning old goals, friendships, and coping skills, relying on influencers’ rapid-transition narratives instead of multidisciplinary assessment and supportive, trauma-informed care.
Although ego can easily hijack gender exploration, an authentic trans self usually develops through slower, relational, and supported processes that honor your full life, not just your gender story. Research consistently shows you consolidate gender identity more durably when others affirm you, especially family and long-term community.
You’re not just “trans”; you’re a whole person. Clinically, that means integrating gender with your history, trauma, culture, and goals, rather than chasing a perfect image.
As you integrate gender into the rest of your life, staying rooted in your own trans identity means tracking what’s stable in you over time, not just what gets validated in the moment. Treat your gender identity journal as data: for 3–6 months, record situations, emotions, and when you feel most affirmed or dysphoric. Over time, these journaling anchors reveal patterns that separate core identity from performance or pressure.
Use concrete markers—legal and chosen name, pronouns consistently used by close others, any medical steps—as reality checks when social feedback swings. Before irreversible changes, pause 30 days and ask, “Is this me, or who I want others to see?” Bring those questions to a small, steady support network and, when possible, a gender-competent clinician.
An “idol” means any created thing you treat as your ultimate source of worth, safety, or meaning. You don’t just value it; you organize your life around it. Clinically, it can mirror unmet needs—attachment, social validation, coherence. Culturally, it carries symbolism that shapes how others respond to you. When it dominates your choices and relationships, it can reinforce trauma patterns and quietly undermine your capacity for flexible, grounded identity.
You’re asking about “identity”; you can treat it as your organized self concept: how you understand your gender, history, values, and embodiment over time. It includes the social roles you inhabit—like “daughter,” “trans man,” or “nonbinary partner”—and how others respond to them. Clinically, we see identity as multifaceted, shaped by relationships, culture, and trauma, and we respect your own account as primary data, not a hypothesis to disprove.
A person becomes an idol when your nervous system lights up around them like a controlled explosion. You don’t just feel personal admiration; you reorganize your story around their image. Through repeated public recognition, curated vulnerability, and constant exposure, you start borrowing their traits as survival tools. Clinically, that’s introjection: you internalize them as a regulating figure, especially if you’ve got trauma, loneliness, or identity instability shaping your attachment needs.
You’re looking at four components: personal, social, role, and relational identity. You build personal identity from self concept, traits, and a coherent personal narrative. Social identity stems from social labels like gender, race, and community. Role identity reflects gender roles and other responsibilities you occupy. Relational identity comes from repeated patterns in close relationships. Clinically, you don’t “fix” these; you support safety, choice, and integration after trauma.
As you move forward, you don’t have to wage war with your ego—just renegotiate its job description. Notice when “being trans” starts to feel like a fragile trophy instead of a living process. Gently ask what pain it might be shielding. With trauma‑aware support, evidence‑based tools, and communities that welcome your rough drafts, you can loosen perfection’s grip, let go of borrowed costumes, and allow your gender story to stay flexible, honest, and fully your own.
 Featured PostsJuly 15, 2026When Fact-Checking Yourself Goes Wrong: A Conservative Influencer’s Viral Humiliation (Parkergetajob on Youtube)
Featured PostsJuly 15, 2026When Fact-Checking Yourself Goes Wrong: A Conservative Influencer’s Viral Humiliation (Parkergetajob on Youtube) Featured PostsJuly 15, 2026Major Policy Reversal, Trump Drops Plans for Federal Restrictions on Transgender Healthcare
Featured PostsJuly 15, 2026Major Policy Reversal, Trump Drops Plans for Federal Restrictions on Transgender Healthcare News and AdvocacyJuly 12, 2026Federal Court Sides With Transgender Military Personnel in Landmark Case
News and AdvocacyJuly 12, 2026Federal Court Sides With Transgender Military Personnel in Landmark Case Featured PostsJuly 11, 2026Beyond the Walls: Identity and Injustice for Trans Women in Men’s Prisons
Featured PostsJuly 11, 2026Beyond the Walls: Identity and Injustice for Trans Women in Men’s Prisons











